When Does a Child Need a Bone Marrow Transplant Instead of Chemotherapy?

Not every child with a blood disorder needs a bone marrow transplant, and not every child can be cured with chemotherapy alone. The line between the two is drawn by specific medical factors, and parents who understand those factors walk into appointments with far more clarity.
A child may need a bone marrow transplant instead of chemotherapy when the disease cannot be cured with chemotherapy alone, has returned after treatment, or is caused by an inherited blood, bone marrow, or immune system disorder. The decision depends on the diagnosis, risk category, treatment response, and donor availability. Here is a simple breakdown of exactly how that decision gets made.
What Is Chemotherapy?
Chemotherapy uses powerful medicines to kill cancer cells or stop diseased blood cells from multiplying. It travels through the bloodstream and targets fast-dividing cells, which is what cancer cells do.
For many children with blood cancers, chemotherapy works well on its own and is always the first treatment tried. It does not require a donor and can often be administered as day care without long hospital stays.
How it is given:
- IV drip into the vein
- By mouth as tablets or liquid
- Directly into the spinal fluid, especially in leukemia (ALL or AML)
What Is a Bone Marrow Transplant?
A bone marrow transplant (BMT), also called a stem cell transplant or HSCT, replaces diseased bone marrow with healthy donor stem cells, rebuilding the blood and immune systems from scratch.
Two main types:
Allogeneic transplant: Stem cells from a matched donor, usually a sibling, parent, or unrelated volunteer. Most common in children with blood disorders and cancers.
Autologous transplant: Your child’s own stem cells, collected before high-dose chemotherapy. Used in conditions like lymphoma. Read more about autologous BMT here.
What the process involves:
- Conditioning phase: high-dose chemotherapy, sometimes with radiation, to destroy diseased marrow
- Infusion of healthy donor stem cells
- 4 to 6 weeks in hospital in a sterile environment
- Several months of follow-up monitoring
Bone marrow transplantation is now widely available across India. Outcomes vary depending on the child’s diagnosis, disease stage, donor match, overall health, and the transplant centre’s experience.
6 Factors That Decide: BMT or Chemotherapy?
1. The Type of Disease
Chemotherapy is usually enough for:
- Standard-risk ALL (Acute Lymphoblastic Leukaemia)
- Early-stage Hodgkin Lymphoma
- Some types of Non-Hodgkin Lymphoma
A bone marrow transplant is recommended for:
- Aplastic Anaemia (severe cases)
- Thalassemia Major
- Sickle Cell Disease with serious complications
- Fanconi Anemia
- High-risk or relapsed leukaemia
- Myelodysplastic Syndrome (MDS)
- Primary Immunodeficiency Disorders like SCID
For inherited conditions like thalassemia and sickle cell disease, a BMT is the only treatment that offers a permanent cure. Chemotherapy manages symptoms but cannot fix the faulty gene.
2. The Risk Category of Leukaemia
Doctors classify leukaemia as standard, intermediate, or high risk based on your child’s age, white blood cell count, genetic markers in the cancer cells, and early response to chemotherapy.
- Standard-risk ALL: Chemotherapy alone. Cure rates are excellent.
- High-risk ALL: BMT is often recommended, especially if specific genetic markers like the Philadelphia chromosome are present.
- AML: Some children with high-risk AML may be advised to undergo a bone marrow transplant after remission, particularly if genetic testing shows a higher risk of relapse.
3. Cancer Coming Back After Chemotherapy
If leukaemia or lymphoma returns after chemotherapy, the cancer has already shown it can survive the medicines. In most relapse situations, a bone marrow transplant is the next step.
A donor’s immune system recognises and attacks remaining cancer cells, a phenomenon known as the graft-versus-leukaemia effect. This is one of the biggest advantages a stem cell transplant for children has over continued chemotherapy.
4. Donor Availability
Every allogeneic BMT needs a donor with a matching tissue type (HLA matching). Doctors search in this order:
- HLA-matched sibling: Best outcome
- Matched unrelated donor (MUD): Found through donor registries
- Haploidentical transplant: Half-matched parent as donor. Now widely available in India, making it possible for nearly every child who needs a transplant to find a donor within their own family.
5. Your Child’s Age and Overall Health
Before any pediatric bone marrow transplant, doctors check your child’s heart, lungs, liver, and kidneys. The body needs to be strong enough to handle the conditioning phase.
Younger children generally tolerate BMT better. Their immune systems adapt more quickly to donor cells, which is why early consultation with a pediatric BMT specialist in Delhi or your city makes a difference in outcomes.
6. Response to Initial Chemotherapy
In many cases, the decision is not made upfront. The typical approach:
- Start chemotherapy
- Assess response after one or two cycles via bone marrow test
- If full remission is achieved and maintained, continue chemotherapy
- If response is poor or relapse occurs, begin transplant planning
This is called risk-adapted treatment and is now the global standard in pediatric oncology.
Expert Insight from Dr. Satyendra Katewa, Pediatric BMT Specialist in Delhi
The decision between chemotherapy and bone marrow transplant is not based on a single test result. Doctors consider the type of disease, genetic findings, response to treatment, risk of relapse, and donor availability before recommending the most appropriate treatment plan. The goal is always to maximise the child’s chances of long-term cure while minimising treatment-related risks.
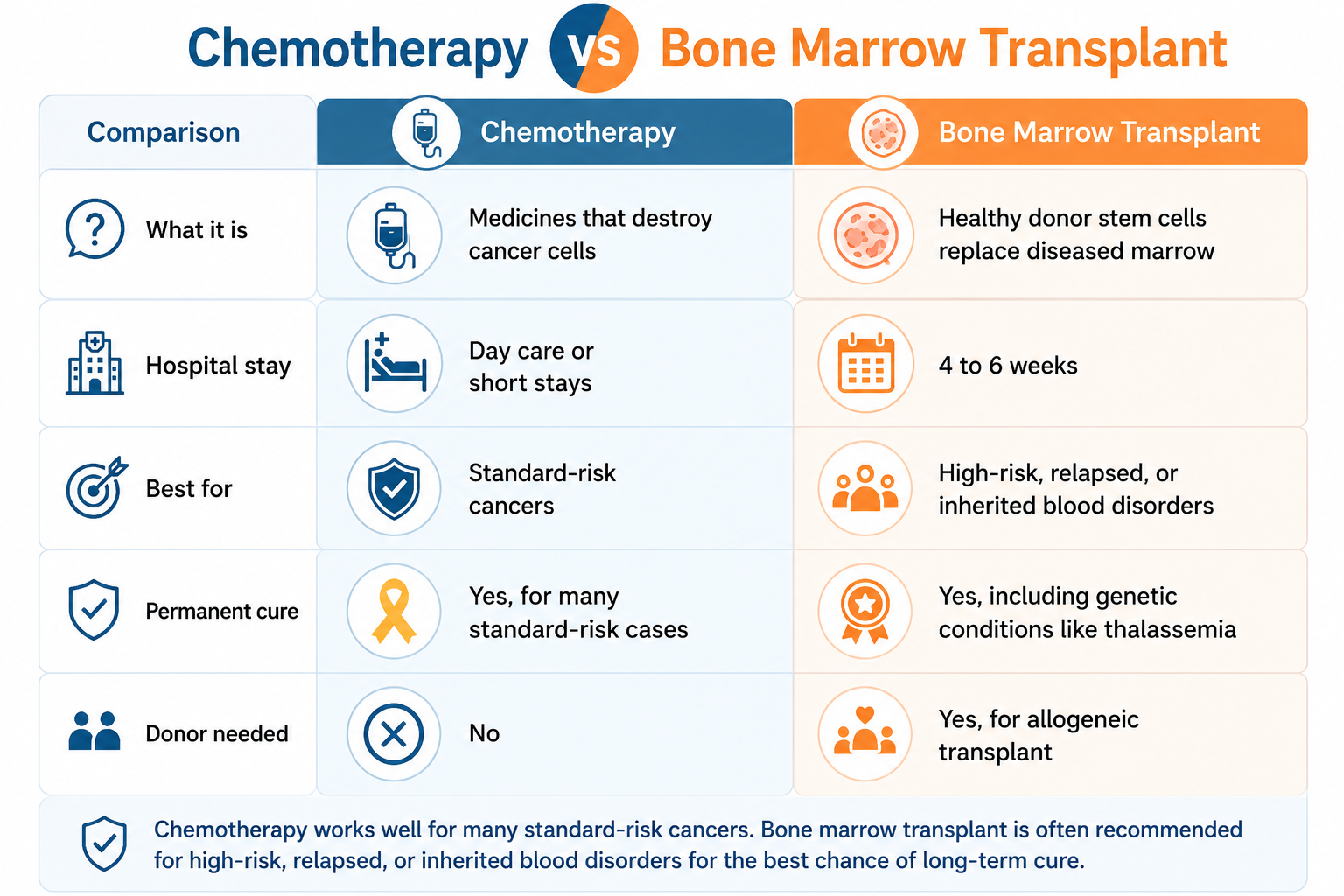
Quick Comparison Table
Questions to Ask at Your Child’s Next Appointment
- What is my child’s exact diagnosis and risk category?
- Is chemotherapy alone likely to be enough?
- If a transplant is needed, how soon should it happen?
- Should we start HLA testing for siblings now?
- What genetic markers have been found in the cancer cells?
The Bottom Line
Chemotherapy and bone marrow transplantation are not competing treatments; they are used for different situations. Many children with blood cancers can be successfully treated with chemotherapy alone. Others, particularly those with inherited blood disorders, bone marrow failure syndromes, immune deficiencies, high-risk leukaemia, or relapsed disease, may require a bone marrow transplant for the best chance of long-term cure.
If your child has been diagnosed with a blood disorder or cancer, discussing both treatment options with a pediatric bone marrow transplant specialist can help you understand the most appropriate path forward.
